Saurabhi Das1, Deepali Bangalia2, Siddhartha Jayantkumar Joshi2.
1Department of Fetal And Paediatric cardiology, Health City Hospital, Guwahati,
2Department of Paediatric cardiology, The Mission Hospital, Durgapur.
ADDRESS FOR CORRESPONDENCE
105 Boys Hostel, The mission hospital, Durgapur, 713201.
Email: Dr.siddharthajoshi@gmail.com | | Abstract | | Supracardiac total anomalous pulmonary venous connection (TAPVC) associated with complete heart block is an uncommon association. We present a case of a 5 month old baby with isolated Supracardiac TAPVC and complete heart block. The patient underwent rerouting of pulmonary veins and an epicardial pacemaker implantation and is doing well on follow up. | | | | Keywords | | Supracardiac TAPVC, complete heart block, epicardial pacemaker. | | | | Introduction | Congenital complete heart block (CHB) is well described in a number of structural heart defects. Corrected transposition of great artery, heterotaxy syndromes are well known association of CHB.1 Totally anomalous pulmonary venous return (TAPVR) can be isolated or associated with other major heart defects. The commonly described association of TAPVR are Tetralogy of fallot, double outlet right ventricle, ventricular septal defect and patent
ductus arteriosus. Association of CHB and TAPVR in a non heterotaxy background has not been described before. We present a case of a 5 month old baby who presented to us with such an association and was successfully treated with pulmonary venous rerouting to the left atrium and epicardial permanent pacemaker implantation.
| | | | Case Report | A five month old baby girl weighing 4.5 kg was brought to our attention with a murmur incidentally diagnosed at vaccination. She had an uneventful birth history and had no significant past or family history. On detailed evaluation she had tachypnea and desaturation (SpO2- 91%).
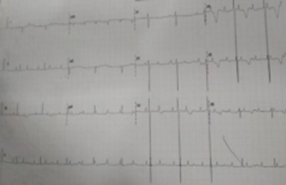
She was noted to have a slow heart rate and a split second sound and hepatomegaly. Chest Xray (Figure 1), showed features of right sided volume overload with plethoric lung fields. 12 lead ECG (Figure 2) revealed Complete heart block with ventricular rate of 65/minute.
Figure 1. Chest Xray showing dilated right atrium and prominent right. Superior vena cava with plethoric lung fields.

Figure 2. 12 lead ECG showing Complete heart block.
On further evaluation by echocardiogram, she was found to have a Supracardiac TAPVR (Figure 3, 4). All the pulmonary veins formed a common confluence which was draining into the right superior vena cava (RSVC) via ascending vertical vein and left innominate vein. There was stenosis at the point of joining of the vertical vein to the left Innominate vein. RSVC drained into right atrium (RA) with an ostium secundum atrial septal defect (ASD) allowing mixture between the right and left atria. (LA) There was also a significant size patent arterial duct.
Figure 3. Four-chambered view showing a pulmonary venous confluence behind LA.

Figure 4. Parasternal long axis view on echocardiography showing all pulmonary veins forming a common confluence behind LA.

The baby underwent corrective surgery with anastomosis of common pulmonary venous chamber to LA, ligation of vertical vein, duct ligation and closure of ASD.. A single chamber epicardial pacemaker was implanted. She had difficult postoperative course complicated by low cardiac output state which was managed by temporary A-V sequential pacing and inotropes. The patient was successfully discharged home on 15th postoperative day and is doing well on follow up.
| | | | Discussion | | Supracardiac TAPVR with complete heart block is a rare association. To the best of our knowledge this association in a non-heterotaxy setting has not been described before in literature. CHB is well known to occur with heterotaxy specifically left atrial isomerism along with pulmonary venous anomaly (reference). Arrhythmias, usually supraventricular, have been amply recorded in asymptomatic patients after anatomically successful repair of total anomalous pulmonary venous connections, and rarely complete heart block results.1 Our patient had no lateralization defect as documented by X-ray chest and abdomen and echocardiogram. We implanted an epicardial single chamber pacemaker. In the post-operative period the patient went into low cardiac output state due to ventricular dysfunction for which she was kept on dual chamber temporary pacing. Permanent ventricular pacing was instituted after 5 days. We would like to highlight two important facts in this case; first she presented with yet undescribed but a very important association of TAPVR. Secondly the single chamber epicardial pacing which was placed during primary TAPVR repair was insufficient to maintain cardiac output in the immediate post operative period because of loss of atrial influence on ventricular ejection which was overcome by temporary A-V sequential pacing. | | | | Conclusion | | TAPVC and complete heart block is a rare association in a normally differentiated heart. It is necessary that all cases should be evaluated preoperatively for rhythm disturbances before the repair. | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
- Saxena A, Fong LV, Lamb RK et al. Cardiac arrhythmias after surgical correction of total anomalous pulmonary venous connection: late follow-up. PediatrCardiol1991; 12: 89-91. [CrossRef]
DOI: https://doi.org/10.7199/ped.oncall.2026.69
|
| Cite this article as: | | Das S, Bangalia D, Joshi S J. Supracardiac TAPVC with Complete Heartblock : An Uncommon Association. Pediatr Oncall J. 2024 Sep 11. doi: 10.7199/ped.oncall.2026.69 |
|