16 Apr, 2020
• COVID-19 should be suspected in patients with new onset of fever, cough or breathlessness.
• The possibility of this infection increases if he resides in or has travelled to a place where there is community transmission of SARS-COV-2 within prior 14 days or has a close contact with confirmed or suspected COVID-19 case in prior 14 days.
• In a health care facility if there is a possibility of suspected COVID 19 patient, infection control measures should be implemented immediately.
LABORATORY TESTING
RT-PCR
• Confirmation of COVID-19 infection depends on detection of SARS COV 2 RNA through reverse transcription polymerase chain reaction (RT-PCR) from different samples.
• Collect nasopharyngeal swab specimen to test for SARS-CoV-2.
• Oropharyngeal or nasal swabs are alternatives if nasopharyngeal swabs are not available.
• Expectorated sputum can be collected from patients with productive cough; however sputum induction is not recommended.
• Bronchoalveolar lavage should be collected from intubated patients.
• The sample should be transported to the testing lab in a viral transport medium (VTM).
• A positive test usually confirms the diagnosis though false positive results are possible.
• If initial testing is negative but there is high suspicion of COVID-19, retesting from multiple respiratory tracts is recommended.
• PCR tests detects viral RNA, and thus indicates current viral infections.
• They are widely being used to diagnose COVID-19 cases and testing suspected COVID-19 patients and contact tracing.
Serologic tests
• According to reports, there will soon have antibody rapid test kits available.
• They detect IgM and IgG antibodies using ELISA. IgM is the first immunoglobulin produced in response to an antigen and detected during early onset of disease while IgG is maintained in the body after initial exposure for long term response
• Spike protein on viral surface that is responsible for viral entry into the host cell, is the main antigen that elicits neutralising antibodies.
• The test use blood samples of suspected patients and give results in 15-30 minutes. Thus they are quicker.
• Thus people who have immunity might be able to venture from their homes safely and particularly important for health care workers to know if they have antibodies.
• It is reported that after SARS infection, IgM antibodies are detected in patient’s blood after 3-6 days and IgG detected after 8 days. AS COVID-19 belongs to same family of viruses causing SARS it is assumed that antibody generation is similar. It is unknown and under study to know how long IgM or IgG antibodies will remain in body after infection.
Biofire filmarray
• Different companies like bioMerieux are developing extended biofire filmarray respiratory panel using multiplex PCR which will include SARS-CoV-2 in addition to other common respiratory pathogens.
• It gives test results in 45 minutes.
• Testing for other respiratory viruses including influenza should be done as co-infection has been reported frequently.
Xpert SARS-CoV-2
In view of current pandemic condition of SARS-CoV-2 and need for rapid diagnostic technologies, several laboratories in different countries received Emergency Use Authorization for GeneXpert SARS-CoV-2 Cartridge. It is fully automated assay and provide results in 45 minutes.
Viral culture
It should not be done from specimens of suspected or confirmed COVID 19 infection for safety reasons.
Laboratory features seen associated with worst outcomes include
• deranged liver enzymes,
• raised kidney functions,
• raised inflammatory markers like CRP, ferritin
• lymphopenia.
• Elevated D-dimer, LDH
IMAGING
In asymptomatic or mild infection imaging is not required.
Imaging is needed in stable patients having respiratory or systemic symptoms, those with respiratory symptoms and in critical patients.
Chest X-ray: is a good first-line radiological examination. It can be used to assess the follow up and for pulmonary emergencies. It is easy to perform using portable systems. It shows bilateral, peripheral, patchy opacities.

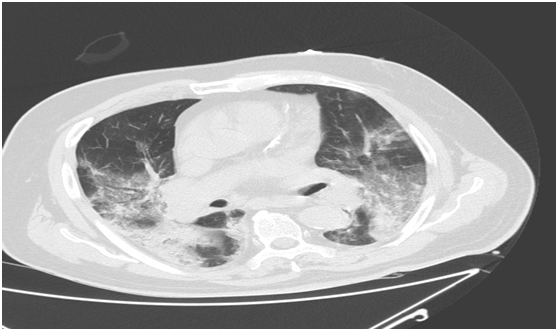
Chest computed tomography: It is useful for lung parenchymal involvement. Along with blood gases it is valuable to predict clinical worsening. Patchy ground glass opacities and consolidation are common features. CT abnormalities have more bilateral and peripheral distribution with lower lobe involvement. Middle aged and older patients have severe lung involvement as compared to younger adolescents and adolescents. With increase in age interlobular septum thickening, crazy paving pattern and large patchy opacities increases. CT Chest is an effective tool for screening. In a study conducted in China, the sensitivity, specificity and accuracy of CT chest in COVID-19 infection were 97%, 25%, and 68 % respectively. The positive and negative predictive values were 97% and 25% respectively. Hence, CT chest can be used for screening and follow up of COVID-19 patients especially in epidemic areas.
Discharge and Follow up
• Discharge criteria and discontinuation of quarantine includes absence of symptoms, clearance of radiological abnormalities and two negative RT-PCR test results 24 hours apart.
• Monitoring of patients who have resolved COVID -19 is also important as discharged patients if still shedding the virus are likely to infect others. Hence self-quarantine up to a month may be advisable.
• Negative RT PCR from rectal swabs were used in SARS-CoV-1 outbreak to determine cure. However in a study of COVID-19 patients it was found that the virus was not isolated from stool sample in spite of high RNA load.
• Serology tests to detect IgG antibodies to SARS-CoV 2 will be useful.
• It is recommended that discharged patients should have follow-up visits after 2 and 4 weeks.
REFERENCES:
1. Chen Z, Fan H, Cai J, Li Y, Wu B, Hou Y, et al. High-resolution computed tomography manifestations of COVID-19 infections in patients of different ages, European Journal of Radiology (2020)
2. Nicastri E, Petrosillon N, Bartoli TA, et al. National Institute for the Infectious Diseases “L. Spallanzani, IRCCS. Recommendations for COVID-19 clinical management. Infect Dis Rep.2020;12(1):8543.
3. www.uptodate.com
4. https://www.biomerieux.com/en/first-3-diagnostic-tests-sars-cov-2-coronavirus-available-biomerieux
5. http://www.euro.who.int/__data/assets/pdf_file/0005/436631/Rapid-communication-COVID-19.pdf
6. The Laboratory Diagnosis of COVID-19 Infection: Current Issues and Challenges. Tang YW, Schmitz JE, Persing DH, Stratton CW.J Clin Microbiol. 2020 Apr 3
7. Ai T, Yang Z, Hou H, Zhan C, Chen C, Lv W et al. Correlation of Chest CT and RT-PCR Testing in Coronavirus Disease 2019 (COVID-19) in China: A Report of 1014 Cases.Radiology. 2020 Feb 26:200642
8. https://onlinelibrary.wiley.com/doi/epdf/10.1002/jmv.25727