Dr Kumud P. Mehta.
Consultant Pediatrician and Pediatric Nephrologist, Jaslok Hospital and Research Centre. Bai Jerbai Wadia Hospital for children. | Antenatal ultrasonography is routinely done in majority of pregnant women in cities. Carefully done antenatal USG by expert sonologist using high resolution equipment (the latest being 3-dimensional one) can detect congenital fetal anomalies. 0.5 - 1% of antenatal USG reveal pelvicalyceal dilatation or hydronephrosis. Majority of pelvicalyceal dilatations resolve over a period of 12-18 months postnatally, however some of them are due to obstruction at pelviureteric junction or posterior urethral valves or severe grades of vesicoureteric reflux that may require surgical interventions. Hence, a pediatrician is faced with the challenge of distinguishing infants with hydronephrosis requiring aggressive evaluation and management from those which can be followed by close monitoring during first 1-2 years of age.
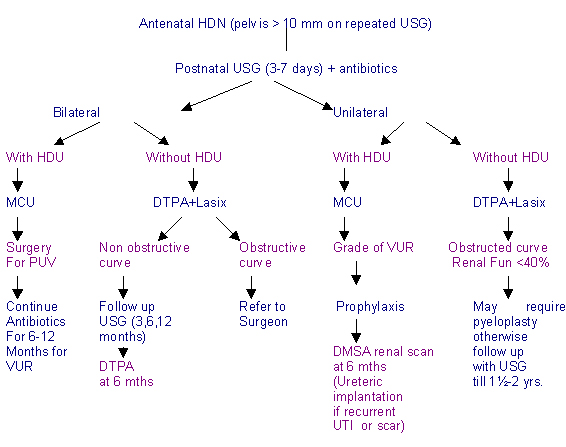
Following guidelines help to decide the rationale approach to hydronephrosis postnatally in antenatally diagnosed HDN :
- Antenatal USG showing > 10 mm AP diameter of pelvis of kidney should be followed every 4 weeks from 20 weeks of gestation of term.
- Postnatal USG to be done between 3-7 days.
- If pelvicalyceal dilatation persists antibiotic prophylaxis is to be started to prevent urinary tract infection. amoxicillin or cephalexin in dose of 25-50 mg/day may be used for 6-12 weeks.
- Bilateral hydronephrosis (HDN) with hydroureter (HDU) and distended bladder in male newborn should be evaluated immediately within 2-3 days. Drainage of bladder by catheterization, micturating cystourethrogram to rule out posterior urethral valves or severe grades of vesicoureteral reflux are important issues requiring aggressive approach. Surgical treatment to relieve obstruction due to posterior urethral valves can prevent damage to kidneys. Many babies with PUV present with delay in passing urine, persistently distended firm urinary bladder and renal lumps due to HDN during the first detailed examination of the newborn. Prune belly syndrome should be ruled out.
- Bilateral VUR does not need surgery immediately. Antibiotic chemoprophylaxis, renal function tests and urine culture to detect acidosis, anemia and urinary infection and treating accordingly form important aspects of medical treatment of bilateral HDN + HDU due to VUR in infancy.
- Bilateral hydronephrosis without hydroureter is commonly due to pelviureteric junction obstruction or impaired drainage and is the commonest cause of antenatal HDN. After the first postnatal USG at 3-7 days after birth, repeat USG at 1 month, 3 months, 6 months and 1 year are useful non invasive tests to monitor PUJ obstruction. If the dilation decreases and renal function on DTPA renal scan is stable, no surgery is required. If AP diameter of Pelvis > 10 mm and worsening of HDN occurs, at 1 month of age Tc 99 DTPA renogram with furosemide is advised to detect obstruction. Surgery is required if clearing of tracer takes > 20 min and renal function is less than 40%.
- Unilateral hydronephrosis with hydroureter needs MCU at about 4-6 weeks to rule out vesicoureteral reflux, ureterocele or rarely ureterovesical (UV) obstruction. Surgical correction is required for ureterocele/UV obstruction.
- Unilateral hydronephrosis without hydroureter is most likely to be due to PUJ obstruction. Repeat USG at 3, 6, 12 months along with Tc 99 DTPA diuretic renogram at 1month and 6 months can identify cases that require pyeloplasty. Poor clearance of tracer (> 20 mins) and poor renal function (less than 40%) require surgical intervention especially if renal function is further reduced by 10% at 6 months. USG shows rapid increase in size of contralateral normal kidney due to compensatory hypertrophy which indirectly indicates deterioration of renal function on affected side. Majority of cases HDN due to PUJ obstruction resolve by 18-24 months and require repeat US and DTPA renal scan to demonstrate resolution.
Follow up for a period of 18-24 months includes periodic growth monitoring, urine cultures, BUN, S. creatinine, (S. electrolytes, blood gases, Hb if indicated) USG and Tc 99 DTPA renal scans till HDN resolves or surgery is done. Bilateral HDN with reduced renal function requires follow up beyond infancy by pediatric nephrologist as these patients can progress to CRF.
 | | | | Compliance with Ethical Standards | | Funding None | | | | Conflict of Interest None | | |
| Cite this article as: | | Mehta K P. APPROACH OF ANTENATALLY DIAGNOSED HYDRONEPHROSIS. Pediatr Oncall J. 2004;1. |
|